Neuromuscular Electrical Stimulation (NMES)
| Author Year;
Country |
Methods | Outcomes |
| Harvey et al. 2010
Australia PEDro=10 RCT Level 1 N=20 |
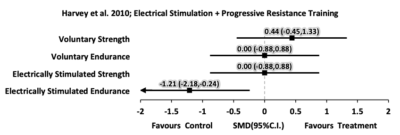
Population: Complete or incomplete SCI patients Experimental group – 7 males, 3 females; mean age 40; mean YPI 3 Control group – 7 males, 3 females; mean age 39; mean YPI 4.Treatment: ES superimposed on PRT 3 days/week for 8 weeks (12 sets of 10 knee extension repetitions against increasing resistance, the first 6 using ES and voluntary contraction and the second 6 using only ES). Outcome Measures: Quadriceps strength and endurance, the performance and satisfaction scales of the Canadian Occupational Performance Measure (COPM), the ES-evoked quadriceps strength (Nm), ES-evoked quadriceps endurance (fatigue ratio), participant perception of treatment effectiveness. |
|
| Effect Sizes: Forest plot of standardized mean differences (SMD ± 95%C.I.) as calculated from pre- and post-intervention data
|
||
| Baldi et al. 1998
USA PEDro=5 RCT Level 1 N=26 |
Population: 26 males and females; age 25-28 yrs; traumatic motor complete; cervical or thoracic lesion level; 15 wks post-injury.
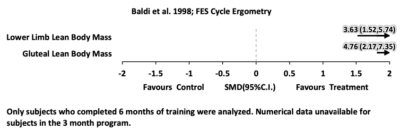
Treatment: Random assignment to 3-6 months of 1. FES-assisted cycle ergometry (n=8), 30 min, 3X/week; 2. PES-assisted isometric exercise group (n=8) (same muscle groups as FES group) for 1 hr, 5X/week and 3 control group (n=9) with no stimulation. Outcome Measures: lean body mass lower limb. |
|
| Effect Sizes: Forest plot of standardized mean differences (SMD ± 95%C.I.) as calculated from pre- and post-intervention data
|
||
| Shields & Dudley-Javoroski 2006
USA Prospective Controlled Trial Level 2 N=7 |
Population: 7 males; age 21-43 yrs; AIS A; C5-T10 lesion level; ³ 6 weeks post-injury
Treatment: PES exercise to unilateral ankle plantarflexion (untrained leg served as a control). Four 4 min exercise bouts, 5 days/week for 1.87-3.05 years. Outcome Measures: Stimulated ankle torque and soleus twitch profiles at baseline and every 6 months up to 3 years. |
|
| Ryan et al. 2013
USA Pre-post Level 4 N=14 |
Population: 14 participants with chronic motor complete SCI (11M 3F); 2 diabetic. Inclusion criteria included: 18-65 yrs of age; AIS A or B classification; normative range of motion in the knee and hip joints.
Treatment: Participants performed RET of the knee extensor muscles 2 times/week for 16 weeks. 4 sets of 10 knee extensions were performed using NMES. Outcome Measures: Plasma glucose and insulin throughout a standard clinical oral glucose tolerance test; thigh muscle and fat mass via dual-energy x-ray absorptiometry; quadriceps and hamstrings muscle size and composition via MRI; muscle oxidative metabolism using phosphorus magnetic resonance spectroscopy. |
|
| Sabatier et al. 2006
USA Pre-post Level 4 N=5 |
Population: 5 males; mean (SD) age 35.6(4.9) yrs; complete; C5-T10 lesion level; 13.4(6.5) yrs post-injury
Treatment: 18 weeks of neuromuscular electrical stimulation resistance training for the quadriceps combined with additional weight around the shin, 2x/week with 4 sets of knee extensions. Outcome Measures: Weight lifted, muscle mass, muscle fatigue |
|
| Belanger et al. 2000
Canada Pre-post Level 4 N=14 |
Population: 14 males and females; age 23-42 yrs; 2 incomplete, 12 complete lesions; C5-T5 lesion level; 1.2-23 yrs post-injury Treatment: Bilateral functional electrical stimulation to quadriceps combined with isokinetic resistance training on left side and unresisted on right; 5 days/week, 24 weeks; each session was 1 hr or until fatigue Outcome Measures: knee torque, endurance |
|
| Kagaya et al. 1996
Japan Pre-post Level 4 N = 5 |
Population: 5 males; age 19-68 yrs; with complete paraplegia (T5-L2 lesion level); 3-60 months post-injury.
Treatment: Subcutaneous PES to various lower limb nerves and muscles for 6 months. Applied at 10 min, 3X/day and gradually increased to 60 min, 3X/day at 10 weeks. Outcome Measures: Muscle cross-sectional area (CT scan), manual muscle test, stimulated muscle torque. |
|
| Hjeltnes and Lannem 1990
Norway Pre-post Level 4 N=4 |
Population: 4 males and females; age 20-36 yrs; Frankel A; T5-T12 lesion level; 3 mos-5 yrs post-injury
Treatment: PES, 4 weeks, 2x/day, 5-10mins, isokinetic resistance to quadriceps muscles followed by 4 weeks, 30 min, 2X/day, 4-5X/day of integrated training of rising and standing. Outcome Measures: Knee extension torque, thigh circumference, CK, collected monthly. |
|
| Gerasimenko et al. 2015
Russia Post-test Level 4 N=10 |
Population: 10 individuals- 5 able bodied and 5 with SCI.
Treatment: Painless transcutaneous electrical enabling motor control (pcEmc) neuromodulates the physiological state of the spinal cord. This method includes electrically activating the spinal circuitry via electrodes placed on the skin overlying the vertebrae of the lower thoracic and/or lumbosacral vertebrae. This waveform consists of 0.3- to 1.0-ms bursts with a carrier frequency of 10 kHz administered at 5 to 40 Hz. PcEmc stimulation was delivered by a 2.5-cm round electrode placed midline at the C5, T11, and/or L1 spinous processes as cathodes and two 5.0 10.2 cm2 rectangular plates made of conductive plastic placed symmetrically on the skin over the iliac crests as anodes. Biphasic rectangular 0.5- to 1.0-ms pulses with a carrier frequency of 10 kHz and at an intensity ranging from 30 to 200 mA were used. Outcome Measures: EMG amplitude |
|
Discussion
Most studies involving NMES and strength evaluated this in individuals with complete or motor complete SCI (Hjeltnes and Lannem 1990; Kagaya et al. 1996; Shields and Dudley-Javoroski 2006). In general, all studies produced beneficial results on muscle size (i.e., reduced muscle atrophy). In addition to enhancing muscle bulk, most interventions also focused on improving muscle function, most notably strength and endurance, as well as contractile speed and muscle fatigue.
Studies with the strongest research design and supporting the efficacy of NMES were conducted by Harvey et al. (2010) and Shields and Dudley-Javorski (2006). Harvey et al. (2010) used an RCT design in persons with both complete and incomplete SCI and found that NMES-assisted exercise increased voluntary quadriceps strength over those that received no intervention. The increase in strength was statistically higher in the experimental group, but it was uncertain if the increase had a clinically important effect. Shields and Dudley-Javorski (2006) employed an experimental non-RCT design to examine the effect of long-term (up to 3 years) NMES exercise to unilateral ankle plantarflexor muscles with the untrained leg serving as a control. This study examined 7 males with complete and relatively recent injuries (~6 weeks post-injury). Peak stimulated ankle torque (i.e, non-voluntary) was found to be significantly greater in the stimulated leg as compared to the untrained leg. The trained side also generated significantly higher torque-time integrals than the untrained side. Other pre-post study designs of NMES-assisted exercise also found increased stimulated muscle forces or torques following training although the participants involved in these studies were generally more chronic (Sabatier et al. 2006; Kagaya et al. 1996; Hjeltnes & Lannem 1990).
Conclusion
There is level 1b evidence (Harvey et al. 2010) that PES-assisted exercise may increase voluntary muscle strength, but the increase may not have a clinically important treatment effect.
There is level 2 evidence (Baldi et al. 1998) that PES-assisted isometric exercise reduces the degree of lower limb muscle atrophy in individuals with recent (~10 weeks post-injury) motor complete SCI, but not to the same extent as a comparable program of FES-assisted cycling exercise.
There is level 4 evidence (Sabatier et al. 2006) that PES-assisted exercise may partially reverse the lower limb muscle atrophy found in individuals with long-standing (>1 year post-injury) motor complete SCI.
