The Stoke Mandeville Spinal Needs Assessment Checklist (SMS-NAC) assesses patient attainment of changes in rehabilitation outcomes through self-rating of perceived physical and/or verbal independence.
It consists of ten rehabilitation domains: physical healthcare (56 indicators), daily ling activities (24 indicators), skin and posture management (26), bladder management (27), bowel management (13), mobility (21), wheelchair and equipment (60), community preparation (33), psychological health (35), and discharge coordination (36).
Clinical Considerations
It is used specifically for patients with a spinal cord injury or disorder. It can be used to identify the patient’s current level of physical/verbal independence, as well as to identify specific targets for rehabilitation goals.
Unlike other rehabilitation outcome measures for people with SCI/D, the SMS-NAC can be scored in relation to physical or verbal ability, enabling patients to achieve full independence irrespective of the severity of their injury and therefore demonstrate for services outcome for people with higher injuries and parity of rehabilitation provision.
ICF Domain
Activities ▶ Self Care
Administration
- Interview-based assessment – The SMS-NAC should be completed with the patient by a member of the multidisciplinary team.
- The scores for each domain are derived by summing the sub-scale item indicators. All items are scored from 0 to 3, with higher scores indicating full physical/verbal independence in or knowledge of that task. Not applicable is used depending on the level of injury, e.g. autonomic dysreflexia. The items that are non-applicable are scored as ‘3’ or fully independent, so that all patients can score fully despite differences in injury etiology. From the summed sub-scales, a ‘percentage achieved’ is calculated for each of the ten domains, ranging from 0-100% with higher scores indicating a greater level of physical/verbal independence.
- Items in each section of the SMS-NAC are hierarchical, so that behavioral items that come first in the section will usually be the areas in which the first rehabilitation goals need to be set, e.g. bed to wheelchair transfers before car transfers.
- Approximately 60 minutes.
Equipment
None
Number of Items
331 indicators
Languages
English
Training Required
No formal training required. However, reading the “Manual” and the “Information for Use Guide” (contacting bht.nsicpsychology@nhs.net) and accessing an SMS-NAC YouTube video (https://www.youtube.com/watch?v=yPt7cvqzSKk) are recommended.
Availability
- A sample of the SMS-NAC worksheet can be found here.
- A copy of the SMS-NAC, license agreement for permission to use, and other materials (such as a “Manual”, “Information for User Guide”, and a scoring tool) can be found by contacting bht.nsicpsychology@nhs.net and/or accessing here (QR code below).

Measurement Property Summary
Number of studies reporting psychometric properties: 4
Interpretability
- MCID: not established in SCI population
- SEM: not established in SCI population
- MDC: not established in SCI population
- Typical values: Mean (SD) scores for each SMS-NAC domain:
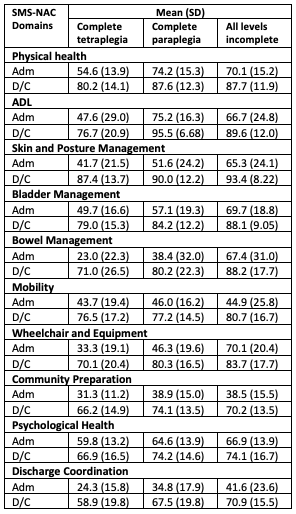
Admission (adm), discharge (D/C)
(Eaton et al. 2022; n=191; 139 males, 56 females; mean (SD) age: 53.0 (17.5) years; 51 tetraplegia complete (C1-C8 A/B/C), 77 paraplegia complete (T1-L5 A/B/C), 67 incomplete (C1-L5 D); mean (SD) time from injury to rehabilitation: 412.6 (2895.7) days)
Reliability – Moderate to High
Number of studies reporting reliability data: 3
- Moderate to High test-retest reliability:
- Overall α = 0.8238
- Subscale α = 0.694-0.904
(Berry & Kennedy 2002; n=43; 38 males, 5 females; mean (SD) age: 42.2 (14.6) years; complete and incomplete tetraplegia and paraplegia)
- Moderate to High internal consistency:
- Overall α = 0.83
- Subscale α = 0.6729-0.9467
(Kennedy et al. 2003; n=192; 147 males; 45 females; mean (SD) age: 40.7 (16.5) years, tetraplegia and incomplete SCI)
-
- Overall α = 0.889
- All subscales α = > 0.7
(Kennedy et al. 2012; n=193; 143 males, 50 females; mean age: 46.6 years; tetraplegia and paraplegia; complete and incomplete injuries)
Validity – Moderate to High
Number of studies reporting validity data: 1
- High correlation between the NAC ADL with SCIM-II (r = 0.873), the NAC Bladder & Bowel with SCIM-II (r = 0.754), and the NAC Mobility with SCIM-II (r = 0.696)
- High correlation between the NAC psychological issues (mood subsection) with HADS (r = -0.726).
- Moderate to High correlation between the NAC psychological issues (full subscale) with HADS (r = -0.523).
(Berry & Kennedy 2002; n=43; 38 males, 5 females; mean (SD) age: 42.2 (14.6) years; complete and incomplete tetraplegia and paraplegia)
Responsiveness
- Responsiveness to change:
- There was an average increase of 60% across all domains of the SMS-NAC (all domains except psychological health demonstrated an increase of more than 20%).
- Weak to moderate differences between rehabilitation scores obtained based on injury level: In nine domains of the SMS-NAC, excluding mobility, there was a significant main effect of level of injury, though the effect sizes ranged from weak (partial η2 = 0.05 for SMS-NAC psychological health, the smallest effect size) to moderate (partial η2 = 0.30 for SMS-NAC activities of daily living, the largest effect size).
(Eaton et al. 2022; n=191; 139 males, 56 females; mean (SD) age: 53.0 (17.5) years; 51 tetraplegia complete (C1-C8 A/B/C), 77 paraplegia complete (T1-L5 A/B/C), 67 incomplete (C1-L5 D); mean (SD) time from injury to rehabilitation: 412.6 (2895.7) days)
Floor/Ceiling Effect
No values were reported for the presence of floor/ceiling effects in the NAC for the SCI population.
Reviewers
Dr. Carlos L. Cano-Herrera, Tyra Chu
Date Last Updated
December 31, 2024
Berry C, Kennedy P. A psychometric analysis of the Needs Assessment Checklist (NAC). Spinal Cord. 2003;41(9):490-501.
http://www.ncbi.nlm.nih.gov/pubmed/12934089
Duff J, Grant LC, Gilchrist H, Jones K. Building and Sustaining Inpatient-Clinician Collaboration in Spinal Cord Injury Rehabilitation: A Case Example Using the Stoke Mandeville Spinal Needs Assessment Checklist (SMS-NAC) and Goal Planning Programme. J Clin Med. 2022; 11:3730. doi: 10.3390/jcm11133730.
https://pubmed.ncbi.nlm.nih.gov/35807024/
Eaton R, Duff J, Wallace M, Jones K. The value of the whole picture: rehabilitation outcome measurement using patient self-report and clinician-based assessments after spinal cord injury. Spinal Cord. 2022; 60: 71-80. doi: 10.1038/s41393-021-00677-7.
https://pubmed.ncbi.nlm.nih.gov/34616008/
Kennedy P, Smithson EF, Blakey LC. Planning and structuring spinal cord injury rehabilitation: the needs assessment checklist. Top Spinal Cord Inj Rehabil. 2012 Spring;18(2):135-7.
https://pubmed.ncbi.nlm.nih.gov/23459415/
Kennedy P, Evans MJ, Berry C, Mullin J. Comparative analysis of goal achievement during rehabilitation for older and younger adults with spinal cord injury. Spinal Cord. 2003;41(1):44-52.
http://www.ncbi.nlm.nih.gov/pubmed/12494320
Wallace M, Duff J, Grant LC. The influence of psychological need on rehabilitation outcomes for people with spinal cord injury. Spinal Cord. 2023 Jan;61(1):83-92. doi: 10.1038/s41393-022-00864-0.
https://pubmed.ncbi.nlm.nih.gov/36435913/
